〈臨床情境〉
檢傷資料
- 病患來診為呼吸短促,血壓或心跳有異於病人之平常數值,但血行動力穩定lmd:後縱膈惡性腫瘤
- Vital signs: T:35.5 P:85 R:22 BP:154/80 SpO2 99% E4V5M6
病史簡述
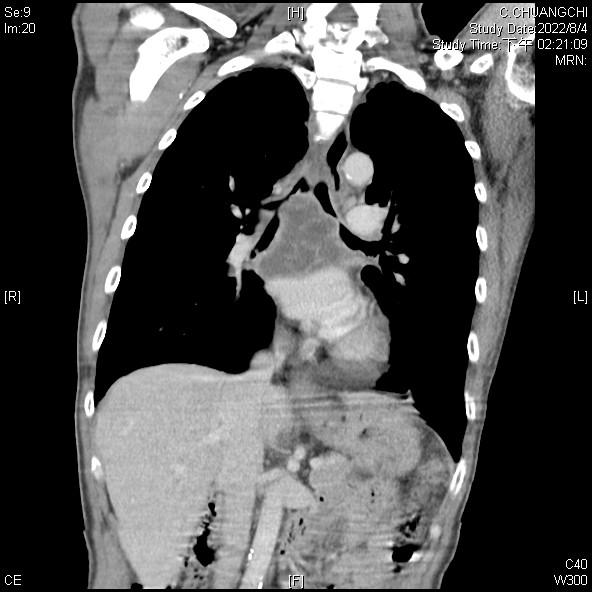
54歲男性無過去慢性病史,主訴漸進呼吸喘一週,合併端坐呼吸及dyspnea on exertion,外院檢查電腦斷層顯示有縱膈腔腫瘤併氣管壓迫,轉至本院做後續治療。
PE: bilateral crackles, no use of accessory muscle
Personal history: smoking 2PPD for 30 years
LMD CT & CXR:


〈初始醫囑〉
檢驗:CBC, WBC/DC, PT, APTT, Sugar, BUN, Cr, Na, K, ALT, CRP, Blood gas, Sputum gram’s stain and culture, Covid-PCR
處置:nasal cannula 5L/min, on IV lock
〈臨床進展〉
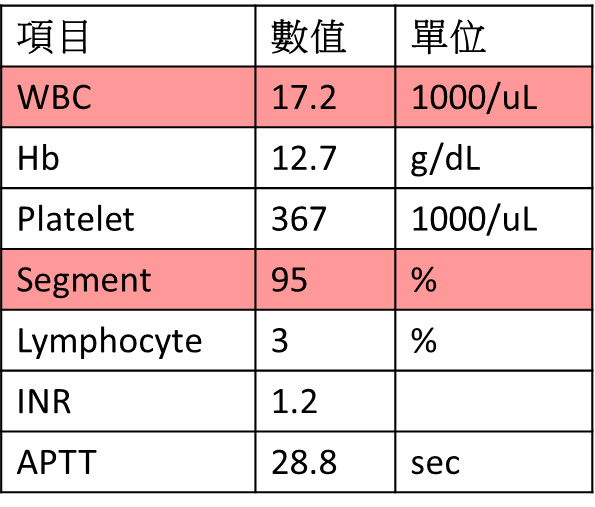
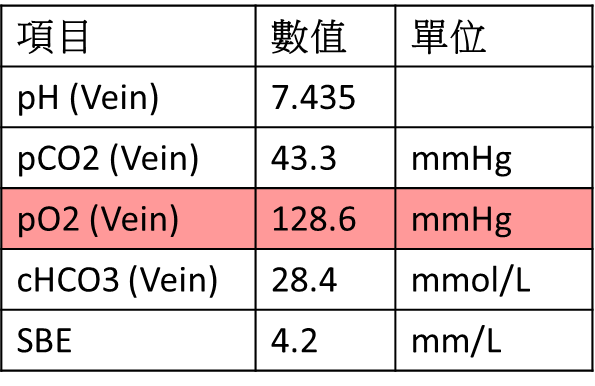
Lab:
會診胸腔外科: 建議做支氣管鏡切片確認病理診斷,安排整體評估後續治療;若臨床出現氣管壓迫可再次照會胸腔科進行置放tracheal stent。
來診16 hrs後: sputum impaction feeling, bilateral wheezing, no use of accessory muscle, stable vital sign

🡪 加化痰藥
來診28 hrs後: dyspnea, orthopnea, stridor and wheezing sound, impending respiratory failure
🡪 Epinephrine inhalation
Consult ENT doctor: Suspect trachea lumen stenosis; No evidence of vocal cord palsy; Airway patent till vocal cord
Consult CVS doctor: secure airway first
Intubation (RSI) with midazolam and rocuronium
Midazolam line and cisatracurium line for agitation
來診72 hrs後: intermittent desaturation, cyanosis, CO2 retention under ventilator support
High peak inspiratory pressure (40mmHg); low tidal volume (214ml)
Arrange bronchoscopy: right main bronchus total obstruction; left main bronchus near total obstruction
Consult CVS doctor: tracheal stent insertion; ECMO support during operation
Post operation day 1: improved ventilator setting
Post operation day 2: treat ventilator associated pneumonia
Post operation day 9: Pathology: poorly differentiated adenocarcinoma
Post operation day 17: immunotherapy for lung cancer
〈Discussion:central airway obstruction〉
Central airway obstruction (CAO): the obstruction of air flow in the trachea and mainstem bronchi
May overlap with upper airway obstruction
Etiology:
Clinical presentation:
Acute: tachypnea, tachycardia, inspiratory stridor, or wheeze
Endoluminal diameter <8 mm 🡪 exertional dyspnea
Endoluminal diameter <5 mm 🡪 stridor
Subacute: dyspnea, cough, hemoptysis, wheeze, weight loss, hoarseness, dysphagia, chest pain
常被誤診為COPD/asthma AE or bronchitis/pneumonia
若bronchodilator, unilateral monophonic wheeze, antibiotics 無效則要想到是CAO
Diagnosis:


CT
Diagnostic flexible bronchoscopy
Pulmonary function test
Treatment:
Oxygenation
Heliox
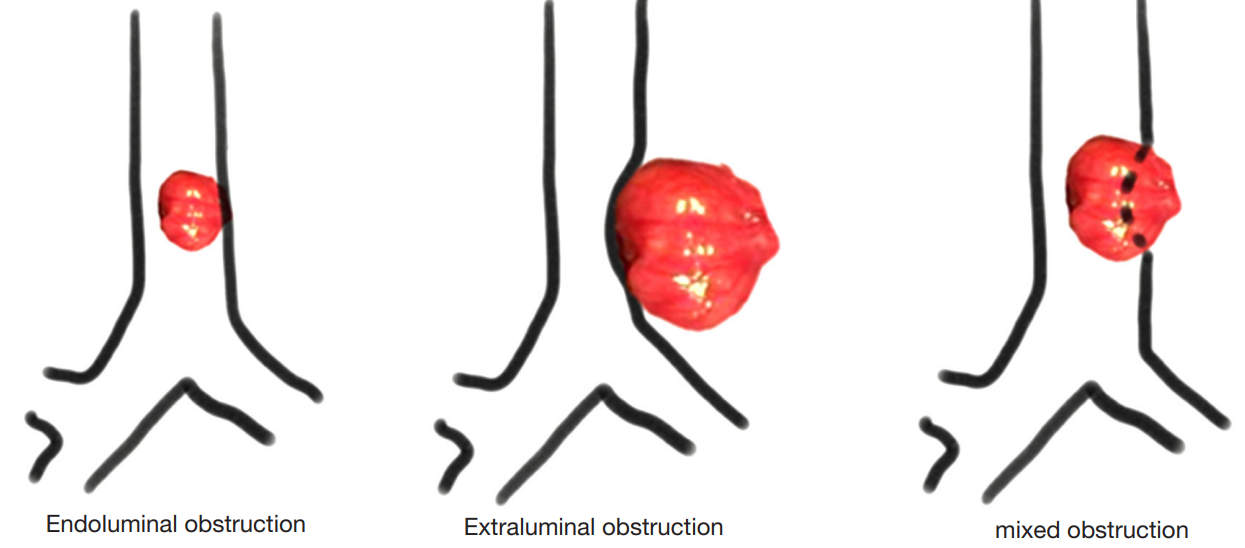
Securing airway (視阻塞位置而定)
Endotracheal intubation 盡可能大號endo (for bronchoscopy), avoid trauma/obstruction
Awake intubation may be safer; with Fowler’s position; short-acting medications for rapid control of general anaesthesia to preserve spontaneous ventilation
Rigid bronchoscopic intubation (oxygenation + ventilation)
ECMO support for bridging to final intervention
Bronchoscopy
Immediately (for foreign body or almost complete airway occlusion)
Within the first 12 to 24 hours (for high grade occlusion in an otherwise stable, ventilated patient)

注意可能共併SVC syndrome
Glucocorticoids
Treat underlying disease
Secure airway
Endovenous recanalization with SVC stent placement
Systemic anticoagulation for thrombus
〈Take home message〉
臨床遇到病患同時出現stridor和wheezing時要懷疑Severe central airway obstruction (CAO)。
若遇到central airway obstruction的病患合併呼吸衰竭須插管時,awake intubation 或使用短效的鎮靜&肌鬆藥物是相對較安全的做法。
遇到central airway obstruction的病患應盡早安排支氣管鏡進行診斷兼治療評估。
若central airway obstruction 病患插管後有ventilation failure 狀況,可考慮ECMO使用。
〈Reference〉
Clinical presentation, diagnostic evaluation, and management of central airway obstruction in adults. Uptodate. Last updated: Sep 23, 2021.
Petersson J, Glenny RW. Gas exchange and ventilation-perfusion relationships in the lung. Eur Respir J. 2014;44(4):1023-1041. doi:10.1183/09031936.00037014
Wood DE. Management of malignant tracheobronchial obstruction. Surg Clin North Am. 2002;82(3):621-642. doi:10.1016/s0039-6109(02)00025-7
Erdös G, Tzanova I. Perioperative anaesthetic management of mediastinal mass in adults. Eur J Anaesthesiol. 2009;26(8):627-632. doi:10.1097/EJA.0b013e328324b7f8
Hartigan PM, Karamnov S, Gill RR, et al. Mediastinal Masses, Anesthetic Interventions, and Airway Compression in Adults: A Prospective Observational Study. Anesthesiology. 2022;136(1):104-114. doi:10.1097/ALN.0000000000004011
Lin J, Frye L. The intersection of bronchoscopy and extracorporeal membrane oxygenation. J Thorac Dis. 2021;13(8):5176-5182. doi:10.21037/jtd-2019-ipicu-08
Abdelmalak B, Marcanthony N, Abdelmalak J, Machuzak MS, Gildea TR, Doyle DJ. Dexmedetomidine for anesthetic management of anterior mediastinal mass. J Anesth. 2010;24(4):607-610. doi:10.1007/s00540-010-0946-x
Williamson JP, Phillips MJ, Hillman DR, Eastwood PR. Managing obstruction of the central airways. Intern Med J. 2010;40(6):399-410. doi:10.1111/j.1445-5994.2009.02113.x
Ernst A, Feller-Kopman D, Becker HD, Mehta AC. Central airway obstruction. Am J Respir Crit Care Med. 2004;169(12):1278-1297. doi:10.1164/rccm.200210-1181SO
Malignancy-related superior vena cava syndrome. Uptodate. Last updated: Mar 23, 2022.
Edited by Ming-Ying, Chiang
留言
張貼留言