
Emergencies related to local tumor effects
判定部位: upper airway(vocal cords以上) vs central airway (vocal cords to carina)
判定來源: endoluminal, extraluminal, mixed
s/s: 喘, stridor, a mass in the pharynx, neck, or supraclavicular area
Direct laryngoscopy不建議!! 因為可能操作不慎造成水腫或出血,使partial變complete obstruction!!
急性處置:
Heliox—typically a 50:50 mixture of helium and oxygen (for cancer-related upper airway obstruction); High-flow nasal oxygen; emergency transtracheal jet ventilation or cricothyroidotomy; awake fiberoptic intubation with a 5-0 or 6-0 endotracheal tube
Bone metastases and pathologic fractures
最常見: 中軸骨(包括頭蓋骨) ,四肢近端
最多來自 solid tumors (e.g., breast, lung, prostate)
X ray只能看出一半 => 建議做CT (with contrast); MRI; bone scan
Management: parenteral analgesics; long-acting oral opioids; palliative radiotherapy (R/T可緩解約80%病理性骨折的疼痛); open surgical repair
Malignant spinal cord compression
20%癌症病人可能發生脊椎骨侵犯,3~6%病人發生spinal cord compression
T spine最常被侵犯
90%病人有背痛症狀; 80%病人原先已知有癌症診斷
=> 所以癌症病人有背痛主訴時,應進行影像檢查s/s: muscular weakness(近端肢體最常見), radicular pain, and bladder or bowel dysfunction, sensory change
影像診斷: MRI with contrast
治療: opioid analgesics, corticosteroids(10mg IV bolus, followed by 4mg PO or IV Q6H), radiation therapy(70%病患有改善), surgery

Malignant pericardial effusion with tamponade
大多沒症狀,有症狀的最多是肺癌或乳癌,也有來自melanoma, leukemia, or lymphoma或電療化療造成
S/S: Dyspnea, orthopnea, chest pain, dysphagia, hoarseness, hiccups, distant cardiac sounds, jugular venous distention, pulsus paradoxus
Tamponade: pericardial effusion + shock (常見的vital sign: tachycardia, hypotension, and a narrowed pulse pressure)
ECG: low voltage, electrical alternans
Echocardiography: diagnosis, evaluation cardiac function
Management: pericardiocentesis; treat cancer (C/T, radiotherapy or intrapericardial chemotherapy); pericardial window; indwelling intrapericardial catheter
預後差,多數病患一年內expire
Superior vena cava syndrome
70% 來自肺癌; 20% 來自淋巴腫瘤; other from intravascular thrombosis or catheter (CVC, pacemaker leads…)
症狀由常見至少見: facial swelling, dyspnea, cough, arm swelling, hoarse voice, syncope, headache, dizziness, visual changes, confusion, seizures, and obtundation
有IICP sign時,病患很可能症狀於一至兩周內急遽惡化CVP=20 to 40 mm Hg (正常2 to 8 mm Hg)
Management:
corticosteroids (evidence只有在lymphoma有效); loop diuretics; head elevation; O2; radiation therapy (75%有效,三天見效); intravascular stents (for thrombosis, fibrosing mediastinitis, mesothelioma); chemotherapy(80% lymphoma, SCLC有效); catheter-directed fibrinolytics and prophylactic LMWH for thrombosis
Emergencies related to biochemical derangement
Hypercalcemia ★★★常考
最常見: Breast cancer, lung cancer, and multiple myeloma
機轉:
1. most commonly by production of a parathyroid hormone–related protein
2. extensive local bone destruction
3. production of vitamin D analogs (lymphoma 最常見)S/S: lethargy, confusion, anorexia, nausea, constipation, general weakness, relative hypovolemia (due to osmotic diuresis)
臨床症狀與血鈣上升之速率快慢有關,而非關血鈣的濃度高,因此血鈣濃度慢性上升的病人相對較無症狀。無症狀者超過14mg/dL才需要治療

Hyponatremia due to inappropriate antidiuretic hormone secretion
何時要懷疑SIADH? Cancer+ euvolemic hyponatremia
最常見:bronchogenic cancer
其他原因: chemotherapy, opioid, carbamazepine, SSRI
Na > 125 大多無症狀,可以限水500ml/day即可
Na 110-125 可能有輕微症狀,可以N/S hydration + furosemide 0.5-1mg/kg PO
Na < 110 可能已經coma or status seizure,需補3% saline 100ml over 10-15min!! 然後再評估,可以視情況再補1-2次!!
Adrenal insufficiency
可能是meta或癌症的藥物治療(chronic glucocorticoid therapy)造成的
S/S: mild hypoglycemia, hyponatremia, hypotension refractory to volume loading and vasoconstriction therapy
Management: 抽cortisol level; IV hydration; hydrocortisone 100mg IV or dexamethasone 4mg IV
Tumor lysis syndrome
血液科的病人最常見!
Hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, AKI, seizure, cardiac arrhythmia, arrest
Management:
灌水到尿有出來; prophylactic allopurinol; EKG monitor; RI + glucose for hyperkalemia & hyperphosphatemia; 除非EKG有變化或seizure否則不要補Ca (會跟P結合成calcium phosphate crystals加重AKI); 洗腎
Emergencies related to hematologic derangement
Febrile neutropenia and infection
定義: ANC < 1000 為neutropenia; ANC < 500為severe neutropenia; ANC <100為profound neutropenia
通常化療後5-10天ANC會降到最低,之後5天就會恢復
臨床評估: (1) 做全套sepsis survey,特別注意catheter entry site、oral cavity、perianal area (注意Digital examination在使用抗生素治療前是relative contraindication!) (2) MASCC risk index或CISNE score算risk
Disposition:
(1) 若檢查檢驗沒有infection evidence且病人評估為low risk則可以口服抗生素OPD follow up (2) profound neutropenia 可預期需要7天以上才會恢復者須住院 (3) 其他survey有異常也建議住院 (4) ANC < 500建議要用抗生素治療; ANC 500-1000看狀況

Hyperviscosity syndrome
Plasma or cellular content 增加造成血液很濃
(plasma: Waldenström’s macroglobulinemia and immunoglobulin A–producing myeloma; cellular: Polycythemia (hematocrit >60%) and leukemia (WBC >100,000)S/S: fatigue, abdominal pain, headache, blurry vision, altered mental status(最常見), cutaneous or mucosal bleeding, Intravascular thrombosis, retinal venous engorgement, dyspnea, fever…
Normal plasma viscosity: 1.7-2.1; normal serum viscosity: 1.4-1.8; hyperviscosity: >4
Management: consult hematologist; emergency plasmapheresis or leukapheresis; 放血phlebotomy 1000ml + N/S 2-3L
Venous thromboembolism (DVT or PE)
Cancer是DVT的risk factor
第一線治療: Low-molecular-weight heparin (其他可選unfractionated heparin or fondadparinux)
單純穩定追蹤癌症者可用DOAC (正在治療癌症者不建議)
Emergencies related to therapy
Chemotherapy-induced nausea and vomiting

For refractory N/V: BZD, dopamine receptor antagonist and antipsychotics
For delayed vomiting (48 hrs-7 days): Neurokinin-1 receptor antagonists
Chemotherapeutic drug extravasation
抽出漏出的藥物、抬高患肢、可能要冰敷或熱敷、可考慮注射antidote (局部注射steroid or bicarbonate沒有evidence!)

Complications due to biologic therapy
注意常見的monoclonal antibodies (機轉:為一種人造的protein,會與T cell 結合,使T cell去殺死癌細胞),Rituximab 可能會引發cytokine release syndrome (CRS)
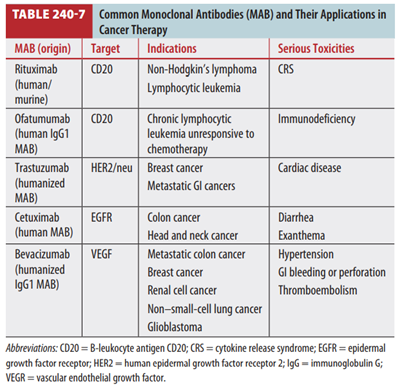
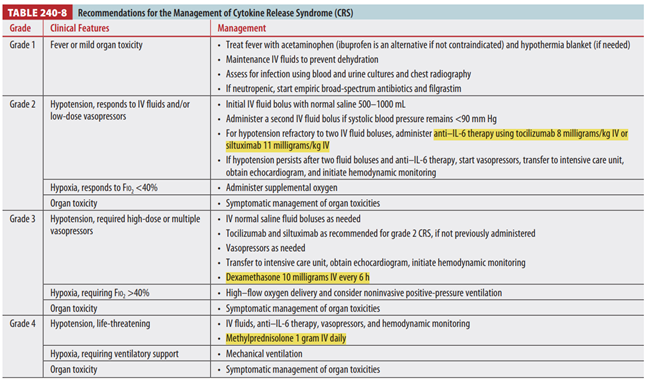
Cytokine release syndrome: T cell過度活化製造過多IL-6,引起身體的嚴重發炎反應,因此治療可以用anti-IL-6 agent (ex: Tocilizumab, siltuximab)。診斷常常難與Anaphylaxis區分。
Immune checkpoint inhibitor therapy: 有些癌細胞可以抑制T cell的作用導致T cell沒有辦法殺死癌細胞,這個療法就是藉由monoclonal antibodies打破這個問題,讓T cell得以恢復功能去殺死癌細胞
常用藥物: ipilimumab, nivolumab, pembrolizumab
Adverse effect:
ipilimumab最多副作用,最常見diarrhea, enterocolitis; nivolumab最常有pancreatitis; 其他可能會有的: Hypophysitis, inflammation of the pituitary gland, thyroiditis, pneumonitis, dermatitis, adrenalitis, nephritis, vasculitis, anemia, and uveitis治療: steroids!! 2nd可考慮anti-TNF-α therapy
考古題:
110.
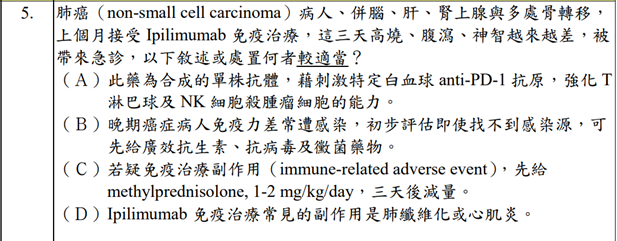
答案: C
A: 是合成單株抗體沒錯,但沒有強化NK cell,也不知道是不是anti-PD-1
B: 沒有要routine給抗病毒和抗黴菌藥物
D: 常見副作用是AGE
109.
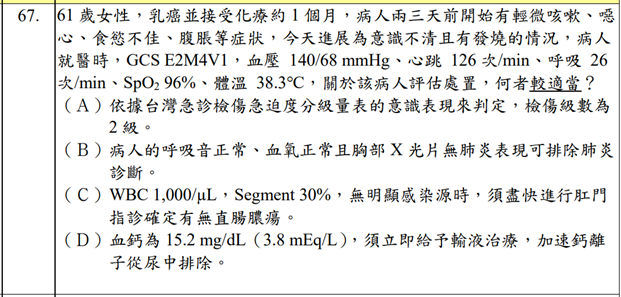
答案: D
A: GCS < 9為一級; GCS 10-13為二級
B: 肺炎有可能症狀只有輕微咳嗽而已,CXR有可能看不出來 (因為化療後免疫系統無法發炎反應所以CXR看不出有infiltration,但實際上有在感染!)
C: Digital要等到有給抗生素後才能做
106.
答案: B
這題應該是考euvolemic hyponatremia
答案: E
A: corrected Ca = 0.8* (normal albumin - pt’s albumin) + serum Ca level
= 0.8* (4-3) + 15.5 = 16.3
E: Calcitonin為rapid onset
答案: E
105.
答案: B
103.
答: D
101.
答: D
A: SVC syndrome 症狀由常見至少見: facial swelling, dyspnea, cough, arm swelling, hoarse voice, syncope, headache, dizziness, visual changes, confusion, seizures, and obtundation
B: 最優先是IVF
C: 症狀表現取決於增加的速度
E: 70% from lung cancer
留言
張貼留言