
Introduction
Pulmonary embolism(PE): 指blood clot進入肺部血管。大部分PE形成原因是從Deep vein thrombosis(DVT)來的。
Venous thromboembolism(VTE) 包含PE and DVT。
依照病因分為provoked, unprovoked
Provoked: surgery, trauma, limb immobility, cancer, infection, chronic disease, estrogen use, pregnancy
Unprovoked(Idiopathic): 大部分在急診診斷的VTE皆是此類。
至少1/3 DVT的病人伴有PE(不一定有症狀); 但在急診被診斷出PE的非臥床病人中只有40%的人同時有DVT。
VTE的危險因子
Immobility: whole-body immobility or neurologic immobility(特別是關節) and with travel >8 hours
Post-surgery: 通常發生在手術後10天以上。其中,手術時間長、Open surgery等也會增加VTE發生的風險。
最常發生VTE的手術有:abdominal surgery to remove cancer, joint replacement surgery, and surgery on the brain or spinal cord in the setting of neurologic deficitsCancer: 分化越差的癌細胞以及tumor burden越大 (如:遠端轉移、癌症接受化療期間),越容易發生VTE。
Pulmonary embolism
症狀
Dyspnea: 最常見的症狀,無法從PE、EKG、CXR解釋的喘。
Chest pain: 第二常見的症狀,常見疼痛位置between clavicles and the costal margin,呼吸或咳嗽會加重。在一些basal lung infarction的病人可能會有referred pain to shoulder,或是mimic biliary pain
其他症狀: syncope, new onset seizure, stroke-like symptoms(paradoxical embolism syndrome)
Physical examination(不一定會在PE病人身上出現)
Vital signs: Tachycardia, Tachypnea, Desaturation
Unilateral limb swelling
Wheezing
其他檢查
CXR: 大部分nonspecific
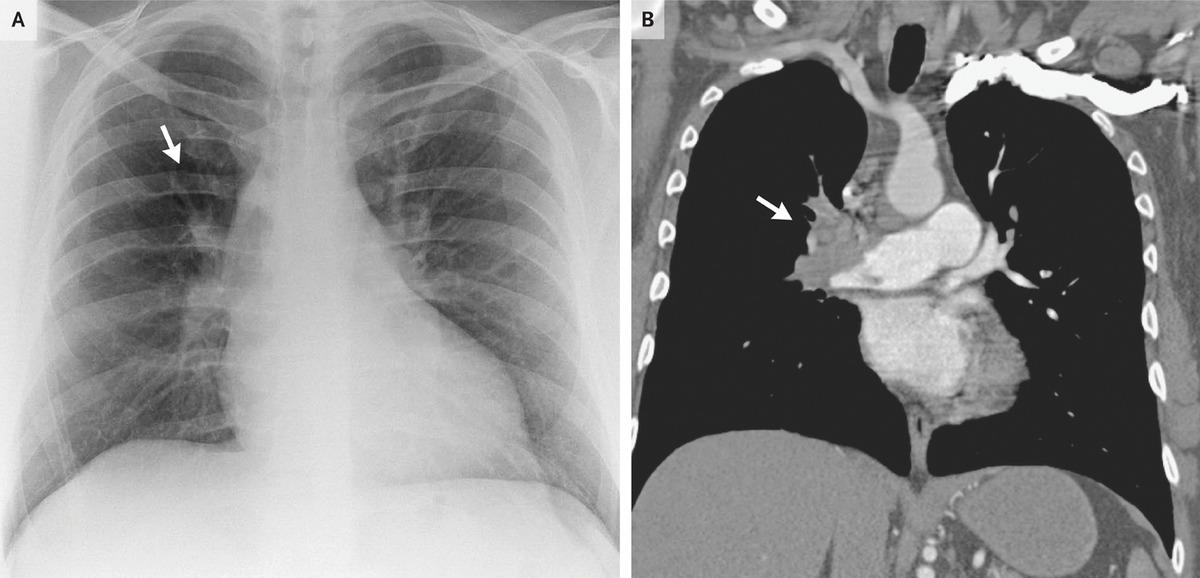
Westermark’s sign (N Engl J Med 2012; 366:e16)
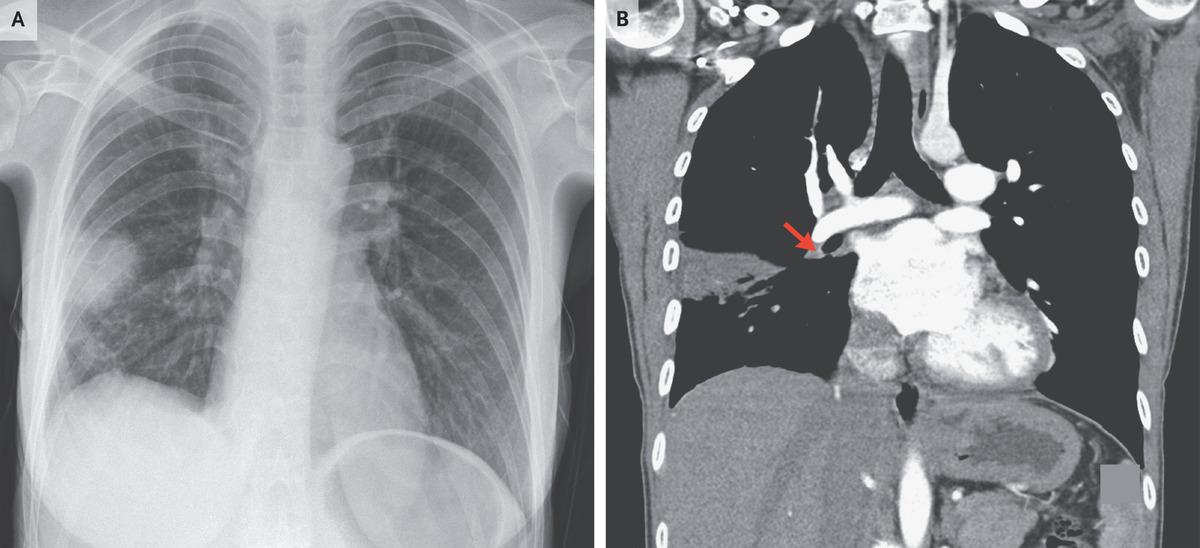
Hampton’s hump (N Engl J Med 2021; 385:1796)
EKG: V1-V4 TWI, incomplete/complete RBBB, S1-Q3-T3 pattern
診斷
當病人有無法解釋的喘、胸痛時,就應該要懷疑
懷疑病人有PE: 計算Wells’ score評估風險
排除:PREC rule (需要9項都符合)
當臨床沒有很像PE,但也無法排除時:D-dimer
D-dimer< 500(or age*10) nanograms/mL: 排除
D-dimer> 500(or age*10) nanograms/mL: 要懷疑PE
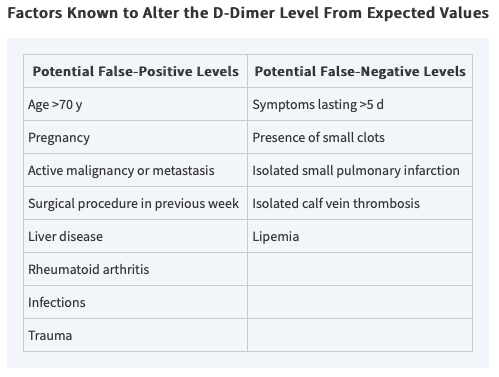
注意D-dimer false positive or false negative
高度懷疑PE: CTA, 用於診斷PE最常見的檢查,在PE當中可以看到filling defect
*PE診斷流程表

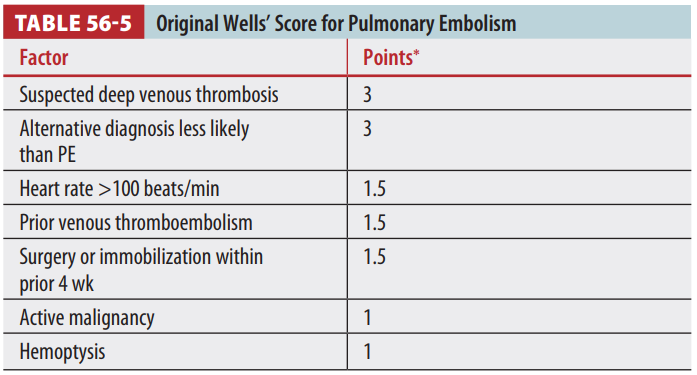
*Wells’ score: 用於懷疑有PE的病人計算PE風險
*PERC rule: 用來排除PE(需要9項都符合)

治療:依照嚴重程度有不同治療方法
1. Massive: hemodynamically unstable (cardiac arrest, SBP < 90, SBP < 100 in HTN, SBP↓40%, desaturation)
*suggest thrombolysis/embolectomy
2. Sub-massive: hemodynamically stable with evidence of RV dysfunction (Trop, BNP, CT, SpO2 <= 90%, Echo hypokinesia)
*strongly consider thrombolysis/embolectomy but need to balance risk of bleeding
3. Less severe: hemodynamically stable with normal RV function
*anticoagulation, inpatient or OPD treatment
以下分述不同的治療方法
Systemic fibrinolysis
適用於無contraindication且屬於massive or sub-massive PE者
Contraindication:
intracranial disease
uncontrolled hypertension at presentation
recent major surgery or trauma (past 3 weeks)
metastatic cancer
藥物: Alteplase(t-PA), 100 milligrams IV over 2 hours
Catheter directed thrombolysis
適用於年紀> 65歲或bleeding risk 較高者
less tPA dose needed(可降低bleeding risk): 約10mg tPA in total
Surgical embolectomy
適用於young patients with large, proximal PE accompanied by hypotension
Mortality rate: 30%
Anticoagulation
LMWH (ex. Enoxaparin): 最常用, dose 1mg/kg BID
UFH: 用於AKI /CKD, extreme obesity, hemodynamically unstable, 用法80 units/kg bolus, then 18 units/kg/h infusion
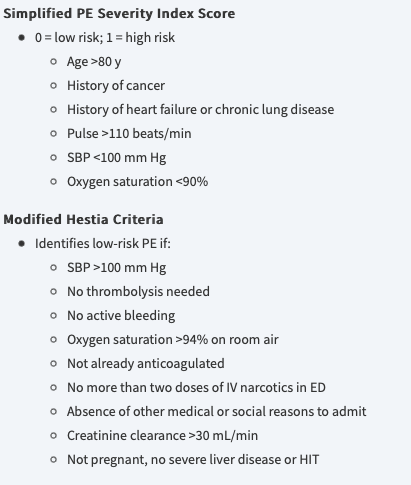
OPD anticoagulation
適用於low risk patient, 可用the Simplified PE Severity Index criteria or modified Hestia criteria來篩選低風險病人
做法: first dose of LMWH (ex. Enoxaparin) or DOAC (ex. Apixaban/Rivaroxaban), 急診觀察24小時後狀況若穩定則回家繼續服藥
Enoxaparin: 1mg/kg BID SC
Rivaroxaban: 15mg BID for 21 days then 20mg QD with food
Apixaban: 10mg BID for 7 days then 5mg BID
Special population: pregnancy
Scores are not validated in pregnancy
D-dimer: always high
No best diagnostic method: CTA(媽媽輻射多) or V/Q scan(小孩輻射多). MRI -> sensitivity too low
Treatment: Fibrinolysis if unstable. Preferred LMWH, UFH if overweight or AKI, CKD.
Do not use warfarin in pregnancy because it crosses the placenta
Deep vein thrombosis
症狀
extremity pain, swelling or cramping (表現可能會像cellulitis)
若是淺層靜脈塞住,可能會導致thrombophlebitis(血栓靜脈炎),造成紅腫熱痛等症狀
Physical examination
兩腿腿圍差超過2 cm (測量處: tibial tubercle下面10 cm)
Homan’s sign: calf vein thrombosis, calf pain occurs with passive foot dorsiflexion (診斷價值不高)
Phlegmasia alba dolens: 嚴重proximal DVT, swollen, painful, and pale or white limb, need aggressive treatment
Phlegmasia cerulea dolens: 嚴重proximal DVT, dusky or blue color limb, need aggressive treatment
診斷
Wells’ criteria
*Original Wells DVT model (不包括最後一項)
≥3 points high risk (75%)
1 or 2 points = moderate risk (17%)
<1 point = low risk (3%)
*Modified Wells DVT model (包括最後一項#)
≤1 point = DVT unlikely; >1 point = DVT likely

治療
治療原則
Treat upper extremity DVT the same as lower extremity DVT
consider removing any indwelling catheters associated with clot
Do not delay unfractionated heparin for thrombophilia testing
Anticoagulation
LMWH (ex. Enoxaparin): dose 1mg/kg BID
UFH: 用於腎功能差且acute DVT病人, dose 80 units/kg bolus, then 18 units/kg/h infusion
Rivaroxaban: 15mg BID for 21 days then 20mg QD with food
Apixaban: 10mg BID for 7 days then 5mg BID
特殊情況:Iliofemoral DVT that causes phlegmasia cerulea dolens
catheter-directed thrombolysis
if not available in 6 hours, consider tPA 50-100mg for 4 hours
需要住院的病人
social determinants
comorbid conditions
the presence of iliofemoral DVT with signs of phlegmasia
PE and DVT 治療藥物總表
歷屆考題回顧





留言
張貼留言