
<臨床情境 1>
30歲男性因被刀刺傷被救護車送至急診,左胸有5公分的撕裂傷正在出血,病人意識清楚,身上無其他外傷。
檢傷生命徵象:T/P/R 35/98/16,BP 73/55,SpO2 99,E4V5M6。
理學檢查:左胸傷口疑似連到心包膜。
初級評估(primary survey):
Airway and C spine protection:可以說話;呼吸沒有異音;氣管無偏移;頸部無活動受限
Breathing and ventilation:血氧濃度正常;雙側呼吸音等大
Circulation and hemorrhage control:低血壓;左胸傷口大量出血且疑似心臟穿刺傷
處理:輸液1L;on large bore;緊急備血及輸血;外傷傷口加壓止血;左胸chest tube insertion;插管;急照會心臟外科醫師
Disability and neurologic status:意識清楚
Exposure and environment control:檢查病患全身;無其他部位外傷
<臨床進展>
因診斷為心臟穿刺傷,在置放胸管及開始輸血後,安排絕對緊急手術送至手術室。


手術報告:
左前胸刀傷4.5公分,合併右心室破裂(撕裂傷3.5公分)、出血性休克及cardiac tamponade。
左側大量血胸併左側內乳動脈(LIMA)損傷。
右心室破裂縫合;左內乳動脈修補;Left side pneumolysis to check bleeding
病患於術後轉至CVSICU,當天拔管;術後第2天轉至一般病房;術後第4天拔除胸管及pigtail引流管;術後第6天出院。
<臨床情境 2>
30歲男性因被車禍被救護車送至急診,病人意識清楚,頭部及腹部鈍傷,頭部擦傷,四肢無其他外傷。
檢傷生命徵象:T/P/R 35.8/52/16,BP 82/64,SpO2 96,E3V5M6。
理學檢查:呼吸淺快但呼吸音對稱;骨盆穩定;腹部沒有壓痛。
初級評估(primary survey):
Airway and C spine protection:可以說話;呼吸沒有異音;氣管無偏移;頸部無活動受限
Breathing and ventilation:血氧濃度正常;雙側呼吸音等大;呼吸淺快
處理:插管
Circulation and hemorrhage control:低血壓;心搏過緩
處理:輸液1L;EKG;備血;FAST;CT
Disability and neurologic status:意識清楚
Exposure and environment control:檢查病患全身;無其他部位外傷
<臨床進展>
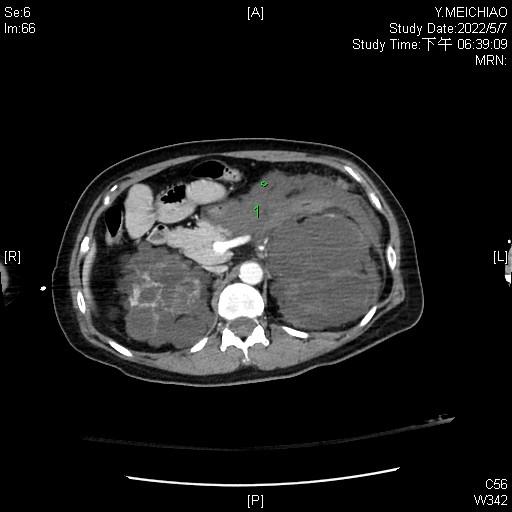
CT:
moderate pericardial effusion
Fluid accumulation around pancreatic body/tail, left perirenal space and left paracolic gutter, likely hemoperitoneum due to rupture of cyst
Contrast medium active extravasation within left kidney, likely rupture of cyst(s).


因懷疑有心臟鈍傷及腹內出血,緊急照會心臟外科及外傷急症科醫師,安排緊急備血及輸血,安排絕對緊急手術送至手術室。

手術報告:
retrosternal soft tissue hematoma
Pericardium: smooth, no hematoma, no active bleeding or oozing
Pericardial effusion: total volume 100 ml, clear.
Distended hematoma at left retroperitonium
Left nephrectomy was done due to nearly total transection of upper and lower pole of left kidney.
病患於術後轉至GSICU,術後第三天進行2nd loop laparotomy exploration;術後第6天拔管;術後第8天轉至一般病房;術後第13天出院。
Penetrating Cardiac Injury
簡介
若外傷受傷部位為the “box”則需要懷疑有心臟損傷。Box上緣為雙側鎖骨,下緣為肋骨下緣,側邊為雙廁鎖骨中線。
多為刀傷或槍傷
simple (single chamber involved) or complex, including injuries beyond the myocardium
發生率最高為右心室(37%~67%)
超過一半的病患會在現場死亡,四分之一病患會在送醫途中死亡
症狀和徵象
Restlessness and refusal to lie down
Beck triad: muffled heart tones, jugular venous distention, and hypotension
Kussmaul sign: jugular venous distention upon inspiration
Pulsus paradoxus
Frequently associated with pneumothorax and hemothorax
診斷
Lab: trauma panel
CXR: widened mediastinum (PA view超過6公分或AP view超過8公分)或合併氣胸或血胸
EKG
治療
Trauma center
Initial assessment: ATLS
FAST
ED thoracotomy: 目擊倒下或是收縮壓小於70 mmHg
Operation
預後
20% survival rate after ED thoracotomy
Good prognosis: 到院時有vital sign、沒有低血壓、穿刺傷預後較槍傷好
Blunt Cardiac Injury
種類
Myocardial rupture
Septal and valvular injury
Myocardial infarction
Cardiac dysfunction
Arrhythmia
Concomitant injury and sternal fracture
評估
ABCDE
EKG
FAST
Cardiac biomarkers
CT or MRI
處置
Emergent surgery
Cath (consider for MI)
ACLS
Edit by Min-Ying, Chiang / Jhi-Hijn Li
Reference:
DynaMed. Penetration cardiac injury.
UpToDate. Blunt cardiac injury.
留言
張貼留言